
Struggling with outer knee pain? A guide to ITB syndrome for runners
Iliotibial Band (ITB) syndrome is one of the most common causes of lateral (outside) knee pain in both runners and non-runners.
For many years, this condition was thought to be caused by friction of the ITB rubbing over the outer knee. We now understand that the pain is more likely driven by compression of a highly pain-sensitive fat pad beneath the band, particularly when loads exceed the tissue’s capacity.
When assessing lateral knee pain and addressing ITB syndrome, the primary thing to look at is load magnitude and running biomechanics.
ITB syndrome can be frustrating. It rarely settles quickly and often requires careful load modification, progressive strengthening and patience to achieve lasting improvement.
In this article, we’ll explore the anatomy of the iliotibial band and its relationship to the knee, its functional role, common symptoms and mechanisms of injury, risk factors and strategies to help you recover and return to activity.
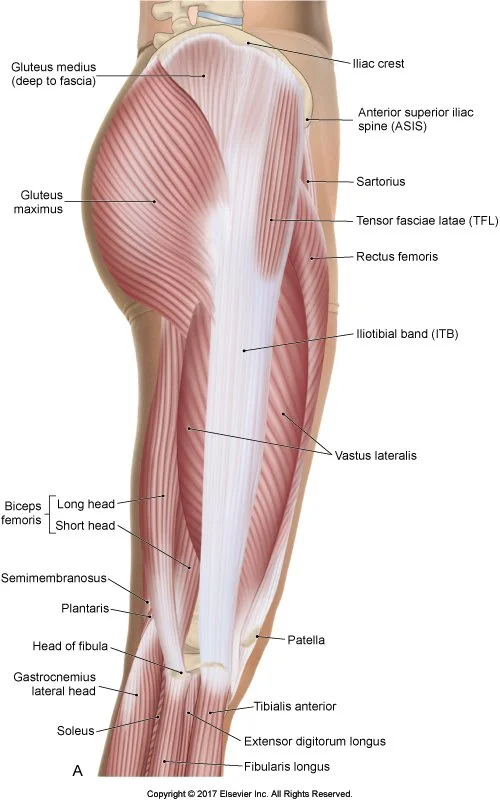
The anatomy of the ITB
Many people are aware that the ITB runs along the outside of their thigh but might be surprised to learn it is a connective tissue and not a muscle.
ITB stands for iliotibial band i.e. ilio = pelvis and tibial = shin bone.
It begins at the pelvis, connecting to the fibres of the gluteus maximus and the TFL muscle (a small muscle located on the outer hip).
It runs down along the outside of the thigh and inserts at the proximal tibia (the upper widened end of the shin bone) at a site referred to as Gerdy’s tubercle, which is a smooth bony projection 2-3cm below the knee joint.
The ITB is firmly attached to the whole length of the femur through fascial connections, though as it has no direct bony attachment to the femur, the ITB can shift anterior or posterior (front to back) as your knee flexes and extends.
The function of the ITB
The ITB is essential for elastic energy storage and release. It is a vital structure for stabilising the pelvis during movement.
The ITB stores 5 – 14% of total work during running. In comparison, the Achilles tendon stores and releases 35% of energy during running.
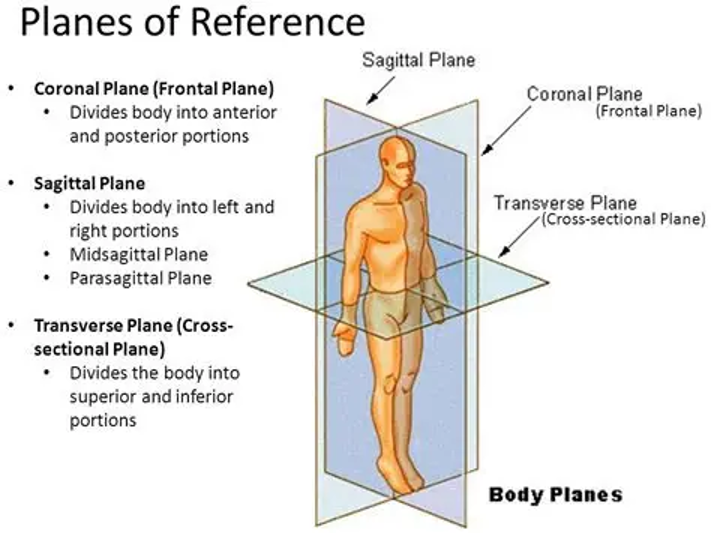
The ITB is an important frontal plane stabiliser for the body. It stabilises against varus (outward pointing) knee torque and the patella (knee cap) against medial dislocation.
The anterior (front) band of the ITB becomes taut with greater knee extension, while the posterior (back) band is taut with greater knee flexion.
The onset of symptoms for ITB syndrome
As mentioned above, although very common in runners, ITB syndrome is the most common cause of lateral knee pain so it should also be considered in cases of non-runners.
The main symptom of ITB syndrome is pain at 25 – 30 degrees of knee flexion (either moving in or out of flexion).
It is common in inexperienced runners who are completing a high weekly mileage or in a rapid increase in downhill running, speed work and overall distance running (such as trail running).
So, what are the risk factors of ITB syndrome?
Training errors present a higher risk factor than running biomechanics, although there are a few considerations.
Below are some points considered NOT to be risk factors for ITB syndrome:
Failing to stretch
Leg length discrepancies
Positive Ober’s test: an examination to test tightness in the ITB and TFL muscle.
Foot pronation
Hip weakness
Weak hip abductors: weak hip abductors do not increase the risk factor for ITB syndrome despite their relationship to the ITB.
A tight ITB is not a risk factor: a compliant ITB results in a compromised ability to store and release energy, and resist varus knee torque.
Shear wave elastography: ultrasound imaging that quantifies tissue stiffness. Note: the stiffness of the ITB does not contribute to ITB syndrome. Therefore, foam rolling is not an effective treatment for ITB syndrome. See further down for more information on foam rolling.
References: Messier S P 1995, Grau S et al IJSM 2008
The mechanisms of injury for ITB syndrome
ITB syndrome occurs when the highly innervated adipose tissue deep below the ITB is compressed. The ITB itself is not highly innervated but the tissue below it is.
This occurs when the ITB is overloaded. The ITB is most loaded with:
Eccentric TFL contractions: i.e. hip extension and knee flexion, particularly when running fast or running downhill.
When varus loads are high: such as the stance leg in downhill running, narrow step width when trail running or running on a slanted surface.
The ITB is loaded least when:
Running uphill: i.e. concentric work is greater than eccentric work.
Walking uphill
Stance leg running uphill
The key is to be careful with high eccentric loads.
What we look for when assessing lateral knee pain and potential ITB syndrome
Investigation into current exercise activity is very important. We want to understand your run history, particularly the overall run volume, downhill running, recent addition of speed work and running on trails.
Other training factors to consider include terrain, incline, speeds, fatigue and surfaces.
Load magnitude is far more important than training volume itself.
We also want to understand how the pain occurs. There is no single diagnostic test to confirm ITB syndrome, but pain is likely reproduced with running (sharp and severe in quality) and descending stairs.
We can however perform some provocative tests to help understand the pain. These include:
Forward step down: this eccentrically loads the ITB and is likely to cause pain.
Decline squat (on a calf board): this test helps to differentiate between patellofemoral joint syndrome (PFJS) and ITB. This test will likely be more painful if experiencing PFJS.
Noble compression test: reproduction of pain at 30 degrees of flexion.
The running biomechanics associated with ITB syndrome
Though the primary issue with ITB syndrome is load magnitude, it is also helpful to evaluate contributing factors due to running biomechanics.
The main consideration when evaluating strain on the ITB during running is what happens when our feet contact the ground (stance phase). This includes not just the feet, but the knee, hip and spine. This is when the most kinetic energy is being absorbed.
A few running gait behaviours can increase strain on the ITB during the stance phase. They often occur together but we will explain them separately.
Overstriding
Overstriding is one behaviour. This involves ‘overshooting’ the ideal landing position of the foot relative to our centre of mass.
What this looks like is a leg that lands with the knee in too much extension (see picture below), such that the tibia is not in a vertical position upon impact.
There is plenty of research to indicate that this is a common factor contributing to running-related injuries.
Striding correlates with running cadence i.e. the number of steps taken per minute.
To limit the tendency to overstride it is best to think ‘run with more steps’, otherwise known as a higher cadence.
This will bring your centre of mass and the landing position of the foot closer together.
The effect is that the foot, knee and hip will all be in an efficient position to absorb kinetic energy and produce forces for push-off.
This may feel like it will slow you down because you are not pushing off with as much effort on each stride, however a high running cadence will also improve your running efficiency and overall performance, once you get the hang of it.
Of course, you will need to have your cadence measured and correlated with the pace you are running at before any adjustments are made.
Narrow step width
Another behaviour commonly seen is a narrow step width (also known as cross-over gait).
This is observed from behind a runner (coronal view) and is when half (or more) of the foot striking the ground crosses over the body’s midline.
Although in part a foot placement strategy, a 2015 study showed that a narrow step width is correlated with overstriding.
Overstriding also plays a role in the increased hip adduction that we often see in conjunction with a pelvic drop (Trendelenburg’s sign) and reduced knee window (dynamic valgus).
It is not solely what happens at the knee, but what we observe happening above (proximal) and below (distal) the knee joint during the stance phase that impacts mechanical stress at the ITB insertion.
The most important thing to note with overstriding, hip drop, knee valgus and a narrow step width is that strength training alone does not resolve any of these behaviours.
Strength is important, yes. However, these are motor control issues and rely on feedback and re-training to improve.
Reference | Reference | Reference | Reference | Reference | Reference | Reference | Reference | Reference
Other conditions that may present like ITB syndrome
There are several other conditions that may present like ITB syndrome. These include:
Patellofemoral joint syndrome (PFJS)
Hoffa’s fat pad impingement
Distal femoral bone stress injury
Gluteal tendinopathy (referred symptoms)
Proximal ITB/TFL enthesopathy
So, how do we rehabilitate ITB syndrome?
It’s key to remember that load magnitude is far more important than training volume. Therefore, the rehabilitation of ITB syndrome should be guided by load management and progressive capacity building.
At the first stage of ITB syndrome – the pain dominant phase – aggravating exercises such as running should be reduced or ceased to reduce irritation.
According to Willy 2023, “The challenge is to reduce abusive loads and irritation of the ITB while maintaining loading as tolerated.”
In the second stage of rehabilitation – the load dominate phase - rehabilitation aims to build the tissue’s capacity to handle load through structured exercise progression.
In this phase, the first step emphasises capacity and control before then introducing higher forces and sport-specific demands.
During running, the body experiences three distinct loads – peak loads, energy storage and release, cumulative loads.
Each of these loads needs to be addressed in a rehabilitation program for ITB syndrome.
Peak loads: should be addressed with heavy, slow resistance training.
Energy storage and release: addressed with plyometric exercises.
Cumulative loading: by a graded return to running program.
Does foam rolling help ITB syndrome?
Despite widespread use, foam rolling does not appear to help with ITB syndrome and may increase compression at the irritated site.
Foam rolling does not address the underlying load capacity issue and is not supported as a primary treatment option.
Injectables and other treatments for ITB syndrome
For ITB syndrome, some practitioners suggest corticosteroid injections may reduce inflammation and provide short-term pain relief, but injectables are generally not a first-line treatment.
There is minimal evidence to support the use of percutaneous needle tenotomy, platelet-rich plasma injection, prolotherapy, topical nitroglycerin and extracorporeal shockwave therapy for the treatment of ITBS.
Other practitioners suggest that ultrasound therapy may also be beneficial is clinically indicated.
Conclusion
In conclusion, ITB syndrome is a compression injury and not a friction injury as originally thought.
Training load errors are what result in this injury and need to be carefully managed in order to recover properly.
It is important to keep as active as possible by treating ITB syndrome with an active load progressive rehabilitation program.
But patients must understand that patience is required as recovering from ITB syndrome doesn’t happen overnight.
Looking into your running biomechanics may also assist in the treatment and recovery from ITB syndrome. Stay tuned for a future post on running biomechanics, we’re well deep dive on this topic.